

ADVERTISEMENT
Ablation of Ischemic Ventricular Tachycardia Using a New Irrigated Tip Catheter
Case Report
A 79-year-old male with an ischemic cardiomyopathy presented with recurrent ventricular tachycardia (VT). He had a history of a prior posterior wall myocardial infarction, and had undergone two prior coronary artery bypass grafting surgeries in the distant past.
Echocardiography demonstrated biventricular enlargement with hypokinesis of the septum and akinesis of the inferior wall, with an overall left ventricular ejection fraction of 30 percent; SPECT imaging demonstrated no evidence of inducible ischemia.
The patient had a Consulta™ CRT-D device (Medtronic, Minneapolis, MN), which had documented multiple episodes of VT at a cycle length of about 480 ms; several of these episodes had been successfully pace-terminated, although antitachycardia pacing (ATP) had accelerated some of these episodes and resulted in appropriate device shocks. The patient initially opted for pharmacologic management; a trial of sotalol was ineffective, though, and the patient proved to be intolerant to amiodarone due to side effects. A decision was made to proceed with an electrophysiology (EP) study in an effort to map and ablate his VT and reduce his overall VT burden.
The patient was brought to the EP lab at the SoutheastHEALTH Heart Center. Bilateral femoral venous access was obtained via the modified Seldinger technique; an arterial line was also placed for continuous invasive BP monitoring. An Inquiry™ deflectable decapolar catheter (St. Jude Medical, St. Paul, MN) was placed in the coronary sinus, and a quadripolar Damato catheter (St. Jude Medical) was positioned at the right ventricular apex.
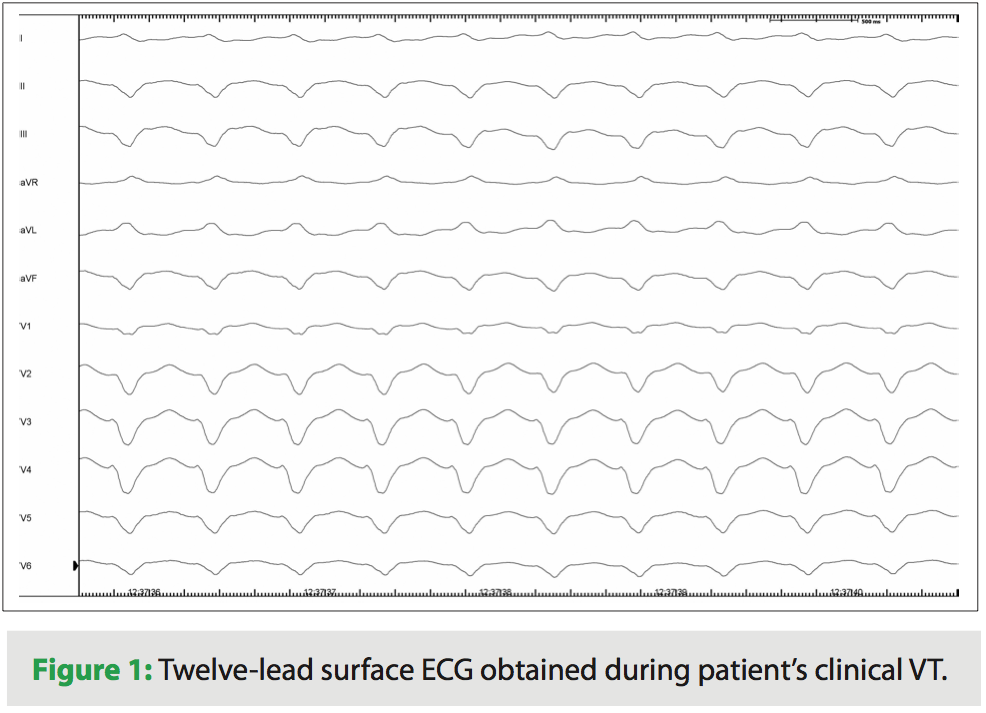 Sustained monomorphic VT with a QRS morphology demonstrating negative concordance across the precordial leads was readily and reproducibly induced via overdrive ventricular pacing (Figure 1); the cycle length of this VT matched that of the patient’s clinical VT.
Sustained monomorphic VT with a QRS morphology demonstrating negative concordance across the precordial leads was readily and reproducibly induced via overdrive ventricular pacing (Figure 1); the cycle length of this VT matched that of the patient’s clinical VT.
A ViewFlex™ intracardiac echocardiography (ICE) catheter (St. Jude Medical) was positioned in the right atrium. Access to the left atrium and ventricle was obtained via a transseptal puncture made with a BRK™ needle inserted into a deflectable Agilis™ sheath (St. Jude Medical) under fluoroscopic and ICE guidance. Confirmation of entry into the left atrium was made prior to advancement of the dilator and sheath assemblies by direct visualization of the needle crossing the interatrial septum at the foramen ovale under ICE, as well as by cineangiography of 1–2 cc of contrast injected through the transseptal needle. Once left atrial access was obtained, an infusion of unfractionated heparin was initiated and the ACT was maintained at 350–400 seconds throughout the remainder of the case. The ICE catheter was used to monitor for the development of any new pericardial effusion.
A Safire BLU Duo™ 4 mm irrigated tip ablation catheter (St. Jude Medical) was introduced into the left ventricle via the Agilis sheath, and a three-dimensional electroanatomic shell and voltage map of the left ventricle was created using EnSite Velocity (St. Jude Medical). Extensive scarring and regions of low voltage were noted along the posterior wall and septum.
VT was re-induced as described above, and a propagation map was created which demonstrated earliest left ventricular activation occurring within the intraventricular septum, with concurrent activation extending anteriorly and posteroapically; however, left ventricular septal activation was noted to be consistently later than activation at the RV apex.
The ablation catheter was subsequently withdrawn into the right ventricle, and a 3D-electroanatomic shell and voltage map of the right ventricle were created. Extensive scarring and regions of low voltage were noted along the right ventricular posterior wall. During VT, a new propagation map was created, which demonstrated involvement of the right ventricular posterior wall scar; entrainment mapping identified a region near the apical edge of this scar as a critical isthmus, with an exact QRS match in all 12 ECG leads during entrainment from this site and a return cycle length <10 ms of the VT cycle length.
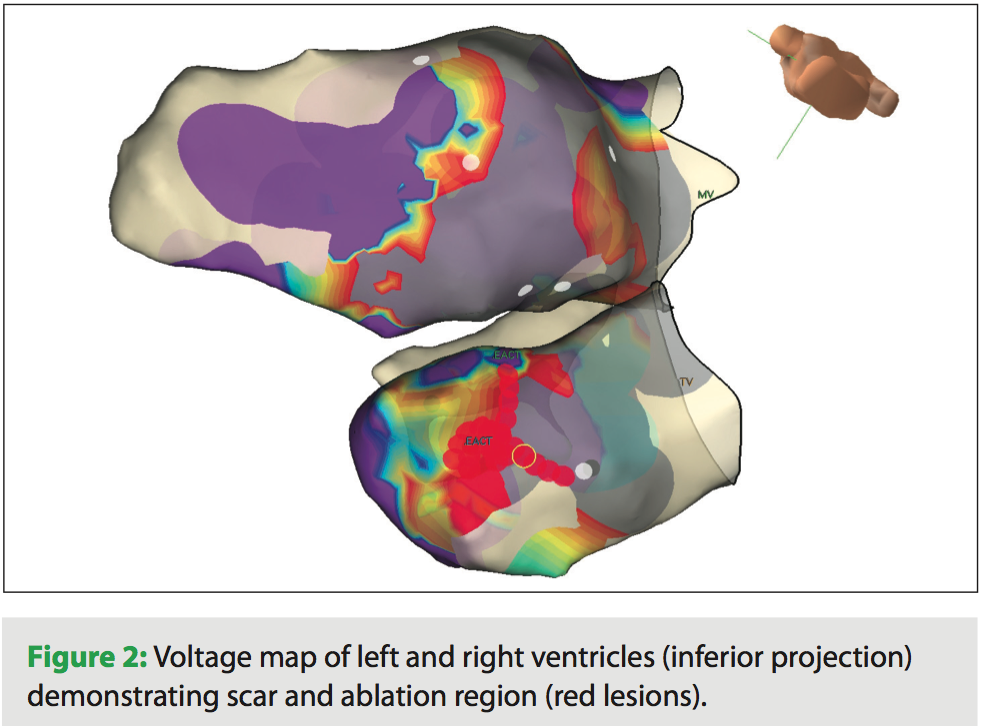 A series of lesions were created at this location during VT at a power setting of 35–50 Watts and temperature cutoff of 45 °C; ventricular tachycardia terminated during RF application. The efficacy of lesion creation during RF application was monitored by observing the disappearance of local ventricular electrograms, as well as by confirming the absence of ventricular capture with high output pacing from the ablation catheter following lesion creation. Lesion locations were tracked via 3D-electroanatomic mapping utilizing EnSite Velocity (Figure 2).
A series of lesions were created at this location during VT at a power setting of 35–50 Watts and temperature cutoff of 45 °C; ventricular tachycardia terminated during RF application. The efficacy of lesion creation during RF application was monitored by observing the disappearance of local ventricular electrograms, as well as by confirming the absence of ventricular capture with high output pacing from the ablation catheter following lesion creation. Lesion locations were tracked via 3D-electroanatomic mapping utilizing EnSite Velocity (Figure 2).
The patient’s clinical VT could not be re-induced on subsequent induction attempts, which included overdrive ventricular pacing at cycle lengths down to 200 ms, and ventricular extrastimuli, delivered at a drive train cycle length of 400 ms and with coupling intervals down to 200 ms or ventricular refractoriness. Although other faster and hemodynamically unstable VTs were seen during these subsequent inductions (requiring DC cardioversion), no attempts were made to ablate these as they did not match any of the patient’s previously documented episodes of spontaneous VT, thereby making their clinical significance unclear.
The procedure was concluded, and the patient was discharged home the next day. His antiarrhythmic drug therapy was discontinued, although he remained on beta-blockers. On subsequent follow-up, the patient has had no further episodes of VT.
Discussion
Catheter ablation has become a standard practice for patients with recurrent ischemic VT, with reported success rates as high as 80 percent in some series.1 The use of an open saline-irrigated tip catheter has been previously described,2,3 and offers a number of advantages including deeper tissue penetration and reduced coagulum formation on the catheter tip. The Safire BLU Duo™ catheter is a next-generation irrigated ablation catheter designed to provide uniform cooling along the entire 4 mm tip length during cardiac ablation procedures. Recently approved by the U.S. Food and Drug Administration in January 2012 for use in the treatment of typical atrial flutter, the catheter features bi-directional deflection for easy maneuverability and 12 irrigation ports for uniform tip cooling — six are distal and six are proximal. In this case report, we successfully employed a Safire BLU Duo™ catheter for a complex ischemic VT case that required extensive mapping of both the left and right ventricles. The catheter demonstrated exceptional torque response throughout the case, which greatly facilitated mapping and lesion delivery. Overall, the Safire BLU Duo™ catheter represents another important tool in our EP lab’s arsenal for treating patients with cardiac arrhythmias.
About SoutheastHEALTH
SoutheastHEALTH is a regional healthcare network with a long history of excellence in cardiac care, serving patients coming from the states of Missouri, Illinois, Tennessee, Kentucky, and Arkansas. In 1966, it opened the region’s first Intensive Care Unit designed especially for cardiology patients, and performed the area’s first cardiac catheterization that same year. Growth in cardiac services and technology continued over the next two decades, and in the mid 1980s open-heart surgery was introduced. In 2008, SoutheastHEALTH opened the doors to the new Arrhythmia and Cardiac Electrophysiology Center. Featuring state-of-the-art technology, including the world’s first deployment of a biplane EP Navigator™ system, the electrophysiology (EP) lab at SoutheastHEALTH has rapidly grown and now performs several hundred EP studies and ablations per year. In 2011, SoutheastHEALTH was ranked second in Missouri for Coronary Interventional Procedures and in the top 10 for Overall Cardiac Services by HealthGrades™.
References
- Sacher F, Tedrow UB, Field ME, et al. Ventricular tachycardia ablation: Evolution of patients and procedures over 8 years. Circ Arr Electrophysiol 2008;1:153–161.
- Nabar A, Rodriguez LM, Timmermans C, Wellens HJ. Use of a saline-irrigated tip catheter for ablation of ventricular tachycardia resistant to conventional radiofrequency ablation: Early experience. J Cardiovasc Electrophysiol 2001;12:153–161.
- Calkins H, Epstein A, Packer D, et al. Catheter ablation of ventricular tachycardia in patients with structural heart disease using cooled radiofrequency energy: Results of a prospective multicenter study. Cooled RF Multi Center Investigators Group. J Am Coll Cardiol 2000;35:1905–1914.


